A series of bills written last year by Michigan State Sen. Mike Shirkey purportedly aimed at “overhauling” behavioral health care in the state are now before a committee to be reviewed. Shirkey, who is also the Senate majority leader, along with Rep. Mary Whiteford, have been pushing this “overhaul” agenda through both houses of the state legislature.
The legislation—Senate Bills 597, 598, and 714, and House Bills 4925 through 4929—would “integrate” mental health services with physical health services. Said to “address gaps” in the state’s mental health care system, the bills claim to be removing a layer of unneeded bureaucracy as well as improving behavioral health services in emergency departments.
“Where you live should not determine access to mental health care, and mental health care, like all health care, must reflect how people live their lives,” said Shirkey. “Through this critical reform, mental health care provided by the state of Michigan will be portable and more accessible, no matter where you call home.”
Whereas the bills in the Senate are sponsored by Shirkey and Sen. John Bizon, both Republicans, the House Bills are receiving bipartisan support.
Whiteford’s plan mostly aims to reduce “administrative costs” to the state by replacing ten public Prepaid Inpatient Health Plans with a “single public or nonprofit administrative services organization.” However, Brian Mills, deputy director of the Michigan Association of Health Plans, claims that Shirkey’s plan is the one preferred by the industry because it gets to the “root cause” of the problems today, forcing the “two different [health] systems to communicate and collaborate.”
Although “pieces” of the proposed legislation are appealing—such as reduced administrative costs and streamlined bureaucracy—critics have been quick to point out that these bills essentially push to privatize mental health care.
The Community Mental Health Association of Michigan and the National Alliance on Mental Illness posted a video back in December to explain the effects of Shirkey’s proposed bills, but much of the criticism is the same for both plans.
Both plans are said to privatize all Medicaid services along with the state’s entire mental health system, handing all decision making over to for-profit insurance companies. Some critics have argued that such legislation is less about integrating care and more about integrating funding.
Some government bodies, though, have already been taking measures to oppose these efforts to privatize mental health services. The Montcalm County Board of Commissioners unanimously voted to approve a resolution opposing these efforts back in January.
Tammy Warner, Executive Director of the Montcalm Care Network, came in front of the Board to ask it to oppose the legislation, which it had voted to do once already in the summer of 2021.
“Everybody thinks that the system is broken, but yet nobody can point out what particularly is broken about it,” argued Warner. She also noted that “for-profit insurance companies pocketed a profit of $550 million in 2020 when people didn’t receive certain health care services that year. They prefer not to provide services because that’s how they make the most buck.”
Warner also pointed out that Gov. Gretchen Whitmer is “staying out of this situation,” which at the time was true. However, since then, Whitmer proposed to “repay up to $200,000 in student loan debt for those working in the nonprofit mental health sector.”
The efforts by the governor are largely focused on offering better care by creating more “access” —which is precisely what Whiteford and Shirkey’s legislation claims to be focusing on as well.
It should come as no surprise that Whitmer’s plan is not so ideologically dissimilar from Whiteford’s or Shirkey’s.
What’s worse is that we know where either of these paths takes us: If measures like Whitmer’s, to create a larger labor force in the mental care industry, are our best (or, worse, only) effort to address this crisis, such labor will—like all industries—“de-skill” itself. Jobs in the mental care field may increase as the demand continues to inflate, but the labor itself will lessen in value.
The care industry as a whole already cannot meet the demands of today. Much like jobs in at-home care, nursing homes, child and elderly care, etc. psychological- and behavioral-based positions will be needed more as people live longer, as more people enter the workforce and stay for longer, and as financial demands continue to increase.
Should we continue down this path, jobs—especially in the private sector—will require less formal training, and eventually there will be low-waged “entry level” therapist positions available.
We’re not even at the point of being able to handle “seeing” mental illness. We may be accepting of mental health when we talk about anxiety or depression, self-care, or even medication; but we rarely accept the underside of mental health, which includes the prison-industrial complex, an ever-growing homeless population (both domestic and those displaced internationally from war, climate change, and pollution), and the clear social aspects of suicidality—such as how things like income and racism affect mental health—which get effaced through ideas of “self-care.”
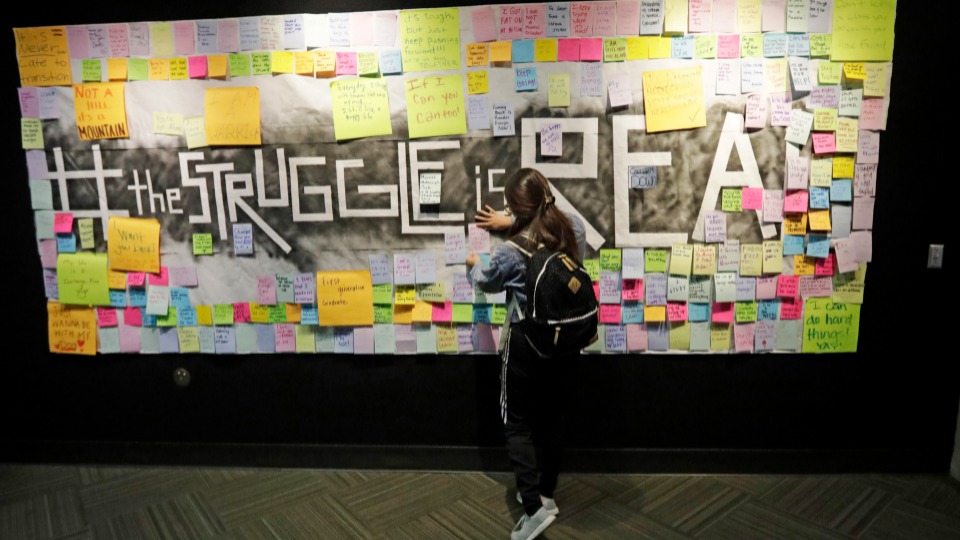
On the one hand, we’re still calling for the “de-stigmatization” of mental health matters; and on the other, we still expect “treatment” to happen behind closed doors, out of sight, and during our “free time.” Although there has been a lot of focus on the former problem, it’s the latter that we take for granted as the “natural” state of handling mental illness.
This is problematic for several reasons, but above all, what gets missed here is that this is what de-stigmatizing mental illness, suicide, addiction, etc. gets us: De-stigmatizing alone results not in structural or social changes, but rather a proper “respect” of mental health at a distance—one that more and more companies are adopting as part of their workplace culture.
Even putting this into terms of “crisis” can be problematic. Indeed, we are in the midst of a care crisis, but the more we focus this into terms of a “health crisis,” the less we are to acknowledge the fact that this is the norm—especially that much of the focus on mental health is solely workplace-focused. Ideas like “burnout” are now commonplace. It seems more that this “crisis” is concerned with garnering more participation than it is with addressing mental illnesses or “burnout” at all.
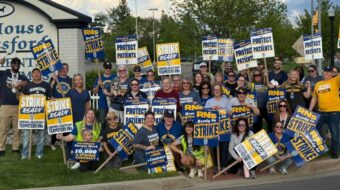
Efforts to privatize Michigan’s mental health system should be resisted at all costs; one poll shows that well over the majority of Michiganders already oppose such legislation. However, that does not mean we should just be grateful for whatever paltry public mental health system is provided, let alone for the solutions the state has offered thus far.
CONTRIBUTOR